
Restoring America's Most Precious Bond
Gender care is fracturing the mother-child bond. But that may be changing.

There is no stronger connection in nature than the protective mother-child bond. This and the entire family unit form the bedrock of civil society.
Yet human arrogance, political expedience, and a compromised medical establishment have tortured that bond by persuading mothers to have their children’s bodies violated in the name of gender affirming care. The interchanging of children's sex organs, by many considered mutilation, has now become primary care.
Equally as destructive as hormone blockers and trans-surgeries is the hiding of critical information from parents. Many schools teach children to keep their transitions secreted from parents. Increasingly teachers lie to mothers and fathers further trivializing parental figures and weakening the mother child relationship.
New York Sanctions Lying to Parents
In 2023 the New York State Department of Education issued a Legal Update and Best Practices directive for creating a safe environment for transgender students. In a long-winded message massage the order was clear. If the student wants you to lie to his or her parents about the transition, or if the teacher feels it is best to lie, then teachers, staff, and vendors are required to lie. In effect NYS is sanctioning the conspiring of teachers and students against parents.

California Empowers Teachers to Lie
In 2024, California Gov. Newsom signed Assembly Bill 1955 into law. The bill maintains that schools and teachers are uniquely qualified to “provide crucial support to LGBTQ+ young people…” Yet these ‘experts’ are in direct conflict with emerging evidence and the move away from transitioning in favor behavioral understanding.
AB1955 references the Trevor Project for guidance. The project was recently defunded by the federal government because their admirable initial mission of reducing suicides has devolved into an advocacy group promoting more transitions. From The Trevor Project home page:
“If you decide that your current gender or sex just isn’t right for you, you may want to make your gender identity fit with your ideal gender expression and presentation.”
While AB1955 does not mandate teachers to lie to parents, by failing to require teachers to tell the truth and by withholding all information “related to a pupil’s sexual orientation, gender identity, or gender expression…” the state is effectively empowering them to lie.
The Trevor Project:

A Jury’s Verdict May Mean the End of Irresponsible Gender Surgeries
Friday, January 30, a New York jury awarded now 22 year old Fox Varian a $2 million judgment in a medical malpractice suit. As a teenager, Fox identified as a male. The jury found that the psychologist, Kenneth Einhorn and surgeon, Simon Chin, rushed through medical interventions for the then 16 year old resulting in a life-changing double mastectomy. Her mother felt pressured into approving the procedure to protect her daughter, who now regrets having it done.
The jury agreed that by fast-tracking the surgery the doctors sidestepped psychological explorations that might uncover possible depression, ADHD or autism.
This case is critically important because it is the first of 28 similar suits to win at trial. Any precedent in this gender surgery case would make insurers think twice before offering liability coverage to the doctors performing them.
In short, this could be the case that unravels the entire gender affirming surgery industry. An industry that had its beginnings when politicians first insinuated themselves into education.
The Rise of Government-Fed Sexual Confusion
Since the first compulsory school attendance law was enacted in 1852, education has suffered from interference by politicians, incompetent ‘experts’, and ideologues chomping to harness young minds to create their version of a Utopian future.
Congress’ 2015 education law, the ‘Every Student Succeeds Act’, marked a shift in the way ideologues invaded classrooms. On the surface ESSA required student performance measures, State Report Cards to inform “stakeholders’, and transparency of per pupil expenditures.
Beneath the surface was a darker story.
ESSA provided government funding for classroom Social and Emotional Learning (SEL) to develop children’s attitudes, behaviors, and competencies like self-awareness and self-management. This became the channel for schools receiving government education money or school vouchers to engage in overseeing children’s mental health.
Promoting Gender Confusion
Social and Emotional Learning and related health curricula, rather than encourage self-awareness, used the mantra of diversity and inclusion to introduce children to terms like non-binary, genderqueer, and pansexual.
While what you are about to read may not yet be happening in your classroom, the government is determined it will soon be part of the curriculum in every district in the nation. The Biden Administration made changes to conflate gender identity with sex discrimination and Health and Human Services released a guidance document titled, Gender-Affirming Care and Young People.
Children were taught why body parts don’t define whether they are a boy or girl and what it means to be transgender, all in the name of mental health education. Youths were told there are dozens of genders and they can pick any pronoun they chose to represent theirs.
To bolster this madness, today children are trained to think of sex and gender as separate categories.
Gender, they learn, is a social construct created by a white male, Eurocentric society whose purpose is to maintain patriarchy and heteronormativity. Sex is determined by whom you go to bed with.
By manipulating definitions, classrooms are erasing 1000 years of medical learning. According to Dr. Leonard Sax, author of Why Gender Matters,
“Today it is politically correct to pretend that gender identity and sexual orientation are two separate entities. While that may be politically correct, the notion is contradicted by the evidence. In reality, sexual orientation is inextricably tied up with sexual identity.”
Rather than concentrate on math, reading, and critical thinking, teachers introduce gender ideology and non-binary lifestyles.
Teens and pre-teens are indoctrinated with ‘gender affirmation philosophy’, the notion that whatever gender a child thinks she is must be accepted as reality. Suddenly, your child’s natural curiosity about the opposite sex, a normal step in the maturation journey, is instead frozen in time and labeled gender dysphoria.
For example, if one day Abby decides she is a boy, a social transitioning begins in which the teacher urges the class to respect ‘his’ chosen pronoun. Abby quickly gets recognition and acceptance for ‘his’ bravery in coming out. If ‘he’ has difficulties winning parental acceptance, Abby can speak to a supportive mental health counselor who explains that ‘gender dysphoria’ is quite normal. The social transition often includes encouragement to make subtle changes in clothing and hairstyles.
Many parents see the changes as just normal phases children pass through. What they do not realize is that instead of being treated as transient, the schools are promoting the phase as a signal for the fundamental life-changing transformation of their child.
Promoting Puberty Blockers
Once a child is diagnosed with gender dysphoria, increasingly schools recommend puberty blockers to “save teen transgender lives.” The argument goes, “since transgender children have higher rates of depression and suicide, we must act now.”
This is the same argument trans-surgeon Simon Chin used to frighten Fox Varian’s mother into ultimately approving the removal of both of her daughter’s breasts.
“This man was just so emphatic, and pushing and pushing… I felt like there was no good decision. I think it was a scare tactic.” — Claire Deacon, Fox Varian’s mother
According to the Mayo Clinic puberty or hormone blockers function differently in males and females,
“In males decrease the growth of facial and body hair, prevent voice deepening, and limit the growth of genitalia.” While in those born female, “the blockers limit or stop breast development and stops menstruation.”
Health professionals point out the blockers are safe and work well. The Mayo Clinic agrees,
“If an adolescent child decides to stop taking GnRH analogues [puberty blockers], puberty will resume and the normal progression of the physical and emotional changes of puberty will continue.”
Hormone blockers are considered so safe, many doctors debate if it is even necessary to provide counseling for teens before prescribing them.
Even the American Academy of Pediatrician accepts the sudden explosion of transgender and gender diverse (TGD) and supports transitioning.
In a show of support, then President Biden’s administration went to court to force doctors to perform transition surgeries regardless of their religious exemptions. While that attempt failed, he went on to propose changes to Title IX regulations that label gender ideology as an anti-discrimination issue. Under the change, schools could begin the transition of children without parental knowledge.
Rachel Levin, Biden’s Former Asst. Secretary of Health claimed,
“Gender affirming care is life-saving, medically necessary, age-appropriate, and a critical tool for health care providers.”
The Dutch Study
Transition proponents point to the Dutch Study as proof hormone blockers are safe and together with transition surgery save lives.
The Dutch study of 6793 transitioned subjects between 1972 and 2015 concluded that gender dysphoria was increasing and the percentage of people who regretted having a sex change “remained small and did not show a tendency to increase.” A follow up showed no increase in suicide rates for transgender women.
But little in these studies applies to what is happening to our children in school today.
The Dutch participants often underwent years of therapy prior to taking blockers. The median age group was 28. Today schools are introducing hormone blockers before children reach puberty, often with little counseling, and in response to an innocent classroom comment.
This rush to proclaim gender dysphoria plus the pressures of the Biden Administration to promote gender ideology through federal agencies is enough to explain the sudden explosion of children identifying as transgender here in America.
Dutch Doctors Don’t Buy the Dutch Study
Ironically, even in Netherlands, the home of the Dutch Study, doctors who provide gender care say they were pressured by long lists of people waiting for gender treatments. Yet we “know too little about the target group and the long-term effects.”
When asked how these hormone blockers would affect the fertility of boys and girls, Dr. Thomas Steensma, of the Center for Gender Expertise on Gender Dysphoria in Amsterdam, said,
“We just don’t know. Little research has been done so far on treatment with puberty blockers and hormones in young people. That is why it is also seen as experimental.”
Puberty Blockers, Are They Really Safe? The Swedish Awakening
Sweden is one of the most progressive nations in the world. It is a leader in environmental activism, gender equality, and one of the first to recognize gender ideology.
A recent Swedish report showed an alarming 1500% increase in gender dysphoria among teenage girls between 2008 and 2018. More shockingly, 32.4% of these girls suffered from anxiety disorder and 28.9% were clinically depressed. The government wanted to know why this was happening.
On April 26, 2019 the Swedish National Council on Medical Ethic instructed government agencies to research global data and learn more about the causes and treatments for child and adolescent gender dysphoria.
After reviewing thousands of studies over an 8-month period, the Swedish Agency for Health Technology concluded:
They could find no study explaining the rapid increase in incidence of gender dysphoria in children and adolescents.
Few studies on gender affirming surgery in general in children and adolescents were found, and only one on gender affirming genital surgery
There are few studies on long-term effects of gender affirming treatment in children and adolescents are few, especially for the recent groups
Almost all identified studies are of lower quality observational type, and no relevant randomized controlled trials in children and adolescents were found.
The Swedish National Board of Health and Welfare changed their guidance:
The guidance has changed from a previously strong recommendation to treat youth with hormones, to new caution to avoid hormones except for “exceptional cases.”
A more cautious approach that prioritizes non-invasive interventions is now recommended, due to recognition of the importance of allowing ongoing maturation and identity formation of youth.
Psychological and psychiatric care will become the first line of treatment for all gender dysphoric youth <18.
Access to hormonal interventions for youth <18 will be tightly restricted.
Treatment eligibility will be based on the criterion of “distress,” and not “identity.”
That last bullet is revealing. Swedish authorities officially recognize that children mature differently and the generally fleeting curiosity about the opposite sex is part of normal maturation.
The Swedish government is not alone in their conclusions.
After their reviews, Finland revised their recommendations for treating gender dysphoria to focus more on therapy and psychological interventions over medical treatments.
Based on the existing literature, the Astrid Children’s Hospital in Sweden altered their guidelines for hormonal gender dysphoria treatments to they will no longer initiate hormonal treatment for gender dysphoria. These cases must take place in a clinical setting with approval of ethical review.
Still the U.S. Government remains insistent on advancing gender ideology.
When the FDA warned that hormone blockers are related to brain swelling, the Biden administration continued to promote them arguing they save children from suicide.
CDC quotes this study, claiming that changing pronouns reduces depression. Unfortunately, it was a small observational study of just 129 people completed in 2011 – 2012, years before the sudden explosion of youthful transgenders.
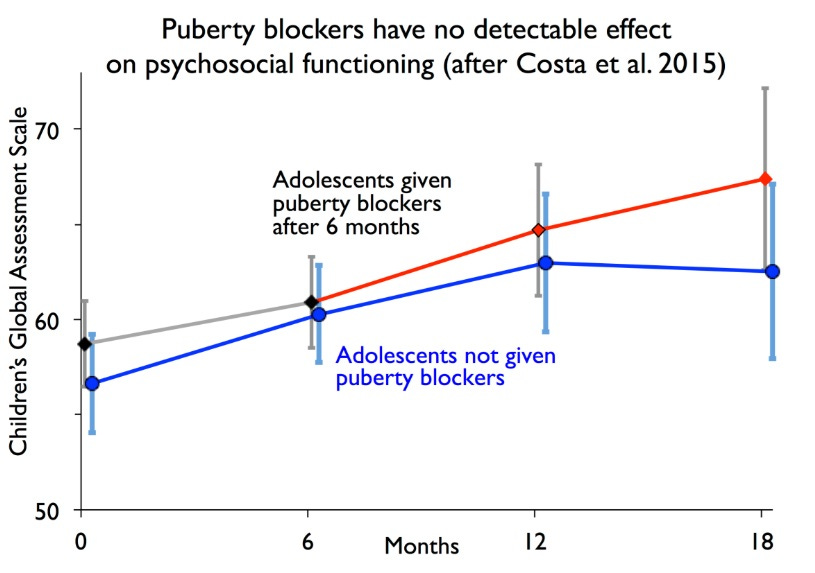
(Above: Effects of Puberty blockers versus no puberty blockers on CGAS psychosocial functioning.)
The Cass Report
In 2020, National Health Service England commissioned British Pediatrician and chair of the British Academy of Childhood Disability, Dr. Hilary Cass, to complete a thorough, independent report on children and young people’s gender services in England.
The investigation ran from 2020–2024 and delivered a scathing verdict on the state of evidence and clinical practice. Here is a summary of the findings:
1. Evidence quality is extremely poor
The review systematically examined every published study purporting to show that puberty blockers, cross-sex hormones, or surgeries improve mental health.
Cass concluded: “There is a lack of reliable scientific evidence about the efficacy or safety of gender interventions for children and young people.”
Essentially, much of the research lacked control groups, had massive attrition bias, and failed to track negative outcomes or de-transitioners.
2. Puberty blockers have no proven mental health benefit
The NHS’s own data showed that children given blockers did not experience measurable improvements in anxiety, depression, or suicidality.
Cass explicitly debunked the widespread claim that blockers “buy time”—in practice, 98% of children on blockers proceeded directly to cross-sex hormones, suggesting the drugs lock in the trans identity rather than pausing it.
3. Mental health problems are central, not peripheral
Most referrals to gender clinics involved complex preexisting issues: autism, trauma, OCD, body image disturbances, and same-sex attraction confusion.
Cass emphasized that dysphoria should be treated in context through mainstream child and adolescent mental health services (CAMHS), not in ideological isolation.
4. Policy and practice changes
The NHS is closing its Tavistock gender identity clinic (GIDS), replacing it with regional centers embedded in normal medical services—not ideologically isolated clinics.
Puberty blockers are now restricted to research protocols only.
The new NHS pathway prioritizes psychological assessment first, not automatic affirmation.
Finally, I Asked AltAI if Gender-affirming Care Reduces Depression
(The mainstream media often claims that “gender-affirming care” including puberty blockers, cross-sex hormones, and surgeries reduces depression and suicidality among people with gender dysphoria.)
“Most of the studies used to justify the claim that gender-affirming interventions reduce depression or suicidality have serious flaws:
“No control groups: Many are “before and after” studies, meaning they measure depression before treatment and again afterward—without controlling for time, expectation effects, or psychotherapy support.
“Short follow-up periods: Results are often measured a few months after intervention, not years. But the post-surgical or post-hormonal “honeymoon effect” is well-documented—short-term mood lifts can quickly wear off.
“Convenience sampling: Participants are typically recruited from gender clinics or activist groups, introducing heavy selection bias.
“Massive loss to follow-up: The majority of long-term outcome studies lose contact with many patients. Importantly, those who detransition or regret often disappear from the data.”
AltAI summarized:
“When independent researchers (rather than ideologically aligned teams) reanalyze the raw data from key studies, they often find that improvements in depression or suicidality *disappear* when controlled for confounding factors such as therapy, family acceptance, or preexisting mental illness.”
In Conclusion
There are many fine, healthy, and happy members of the transgender community who are grateful they made the transition. But these are not representational of what occurs in schools today. Children are being coaxed into alternative lifestyles, plied with experimental protocols, and robbed of the opportunity to mature in their own way. This may be the greatest annihilation of hope for the future we have ever known.
What Can You Do?
The first step is to realize that the government is not your ally. While there are good people in classrooms and in government, they are not fully able to protect your child. The gender ideology and trans obsession we see in schools started in Washington and, if it is not in your school now, it will be soon.
With that understanding, there is much we can do to help our next generations.
Homeschool your children or grandchildren. Chances are there are homeschooling families in your own neighborhood. Reach out and ask them for help with your journey.
Know what your child is learning. If your children are in school, attend school board meetings, meet with the principal, mental health professionals, and teachers to discuss their attitudes toward gender topics. If you have concerns, take your child out of the school. You are not going to be able to change their minds. This is a constant effort as new guidelines are breaking every day.
Maintain a close trust relationship with your children. Remain a strong influence in your children’s lives. I know this sounds obvious, but increasingly schools, movies, entertainers, games, libraries, colleges, medical associations are influencing the way your child thinks and behaves. In many cases transition is taking place without parents’ knowledge.
Interview your doctors and other caregivers. Find out where they stand on gender dysphoria, puberty blockers, and social transitioning. If their position conflicts with yours, find other providers.
Build community networks of like-minded people. This allows the comfort of having others around you and offers a trusted social network for your children. Working together multiplies resources for helping children, keeps people informed about what is happening in schools, and can be the foundation for forming groups to educate more parents.